


Cannabis Use Report re: Primary Care Patients in Los Angeles
Cannabis Use Report re: Primary Care Patients in Los Angeles
A cry for help from primary care patients: 1/5 want more than just primary care

A New Perspective on Cannabis Use in Primary Care
A new study was just published in JAMA yesterday, titled "Cannabis Use Reported by Patients Receiving Primary Care in a Large Health System." This study takes a close look at how common cannabis use is and reports the potential associated risks among adult patients at a university-based health system in Los Angeles, California. Conducted between January 2021 and May 2023, the research aimed to uncover patterns of cannabis use, which they then label (without second-guessing) as meaningfully correlated to risk factors for Cannabis Use Disorder (CUD), and they surface some generalized reasons why the patients they’ve surveyed are using cannabis.
The study screened 175,734 patients with an average age of 47 years. Among them, 17% reported using cannabis in the past three months. Interestingly, 34.7% of these cannabis users were what they defined as “at moderate to high risk for CUD” (spoiler alert: this is mostly bologna). The study found variations in cannabis use and (what they inappropriately call) CUD risk based on age, gender, race, employment status, and neighborhood disadvantage levels.
My Insights and The Holes I see
The findings revealed some noteworthy insights. For instance, cannabis use was more common among younger patients (31% in the 18-29 age group) and males (20%), both of which match up with other data sets. The number they got for adults aged 60 years and older was 8.5%—a bit low, I think, for what I see at CED Clinic and from what I would expect. They used a computer survey, and 15% of the population they serve didn’t even fill out the survey (probably a solid representation of older technophobes). Interestingly, those living in the most socioeconomically disadvantaged neighborhoods had a lower prevalence of cannabis use (13.8%) but a significantly higher risk for CUD (1.4 times higher) compared to those in less disadvantaged neighborhoods. Given that public health data tells us something very different about lower SES groups (namely that they use way more cannabis than the general population), this suggests that those groups either aren’t fairly represented or aren’t revealing this particular truth that we see popping up in other research.
These results aren’t telling us anything incredibly outlandish or scandalous, but they do highlight the complex relationship between individual characteristics, neighborhood factors, and cannabis-related consumption within primary care. The takeaways shared by the authors emphasize the need for “tailored interventions” and support for “at-risk populations” to address these disparities effectively. While they don’t explicitly call cannabis bad, they point to increasing consumption as associated with increasing risk of addiction and the need for intervention and treatments, although they don’t name any or explain why these are concerns—this assumption is treated as inherently obvious.
The BIG “oops”: Questionable Validity of CUD Diagnosis
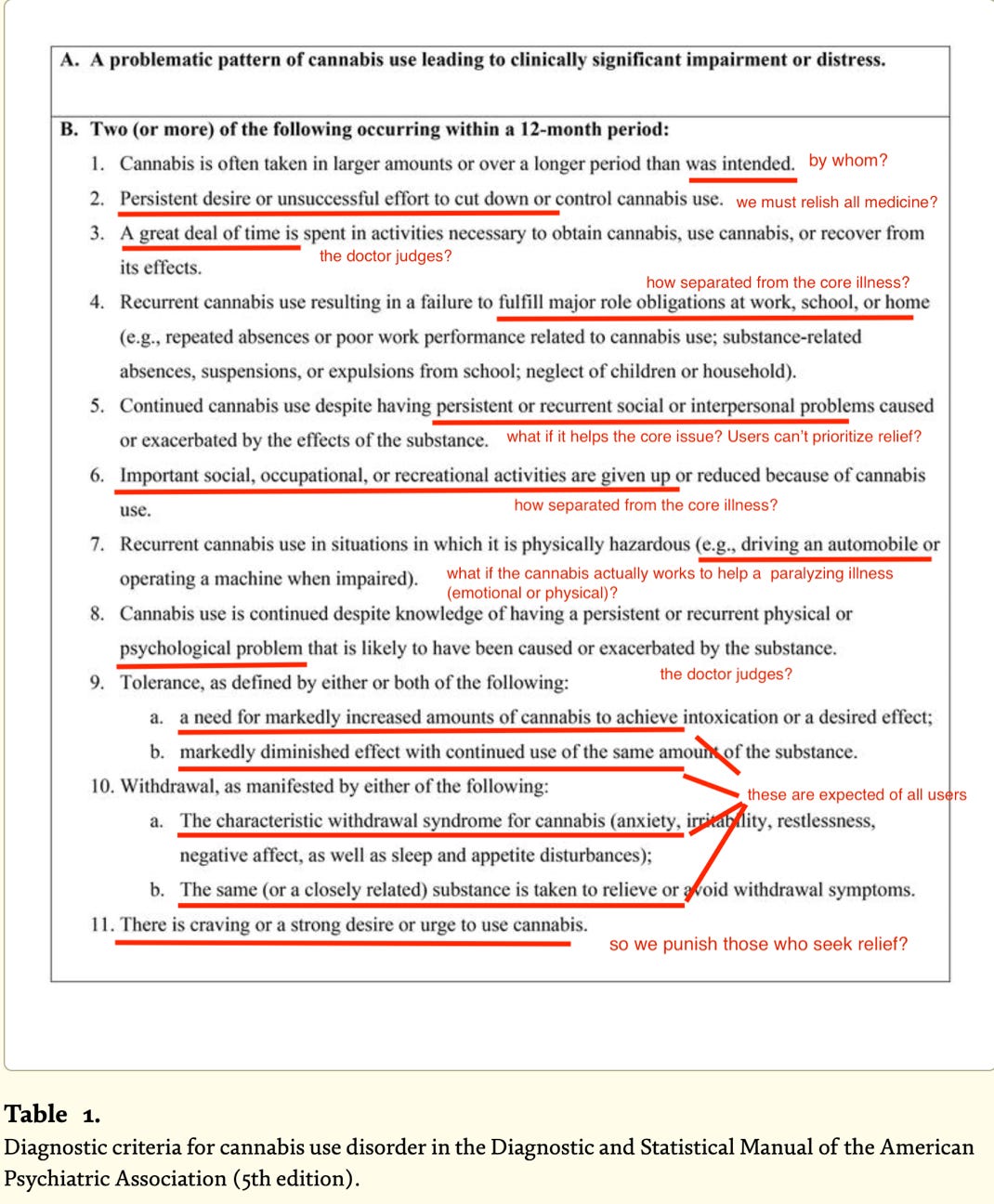
I generally have a deep aversion to the diagnosis of "Cannabis Use Disorder" (CUD). As you can see from the following image that outlines what CUD is (officially) within the medical system, and with my red-lining to highlight the issues I see. For those who are even slightly skeptical or logical, the criteria for such a diagnosis are at best questionable.
Even if we accept that the researchers are attempting to measure cannabis consumption in general, without explicitly labeling it as harmful or even suggesting what it may or may not mean, this study has several elements that are half-baked or based on total leaps of judgment:
Validity of CUD Diagnosis Using ASSIST: A fundamental concern is the use of the “ASSIST” screener to diagnose CUD, which is threaded throughout the article. The ASSIST is a tool that includes questions about cannabis, it is a general instrument designed to assess several different types of substance use disorders. It lacks the detailed focus on cannabis users' specific characteristics. More specialized tools, like the Cannabis Use Disorders Identification Test-Revised (CUDIT-R), provide a more comprehensive assessment specifically for cannabis use disorder - whether or not CUD is even a thing to begin with. Even if we accept CUD as a legitimate diagnosis, the ASSIST does not cover the nuances of CUD symptoms as outlined in the DSM-5, such as craving, withdrawal, and unsuccessful attempts to cut down. Using ASSIST as a direct measure of CUD is clearly inadequate (see the DSM criteria and my issues, attached).
More - check this nutty element out: the researchers, for no apparent reason (none reported anyway) adjusted the cutoff for what defines “mild,” “moderate,” and “severe” CUD, raising the symptom threshold from 4 to 8 (one must meet 8 criteria not merely 4). Ok, scientifically, this just seems arbitrary and capricious. We don’t just do that in research.. unless there is a reason. Now, think through this with me: Consider what might have happened if they didn’t do this. Had they not changed the criteria, the analysis would likely have shown an even crazier, much higher prevalence of CUD, potentially undermining the study's credibility even further, because it would simply appear that everyone that they looked at had CUD (“ah! the monsters are coming, the monsters are coming!”)
To me, the adjustment that the researchers made unveils a truly important takeaway: even patients inside of a “supportive” environment like primary care are heavily reliant on cannabis for symptom relief. To my eyes, this underscores a critical issue that is seen throughout our medical system, which is that doctors are NOT adequately meeting patients' needs for managing anxiety, sleeplessness, pain, and other symptoms. THIS is the important take away, and relevant national news that just isn’t discussed loudly enough. We are unhappy with our care system, and not shy to do what we feel is right by ourselves.
The Need for Informed Conversations
I have to give the study credit for acknowledging some important opportunities that the data presents, namely the need for informed conversations. Healthcare providers must integrate discussions about cannabis use into routine care, and allow patients the comfort and space to communicate their experiences openly. Patients are clearly enjoying cannabis in huge numbers. Their doctors deserve (really, need, to be able to serve patients with full information) to understand why patients choose cannabis over conventional treatments and be informed about both the risks and benefits of cannabis. This will lead to better care, better management strategies and support systems for cannabis consumers -which is a big number of people, whether their use is “medical” or “ non-medical” (the study does identify that this arbitrary naming seems largely meaningless, almost everyone is using cannabis to treat symptoms).
Addressing the Knowledge Gap
Few reading my work are unaware that there is a meaningful knowledge gap in the scientific understanding of cannabis's benefits and risks. On the clinical use side, much more robust clinical research is needed to provide clear guidance on cannabis use and its long-term effects. There is surely a gap in what doctors know and how they can “be there” for their patients. Cannabis has been mainstream forever, but we are living through the age when it is finally coming out of the shadows, as this study clearly spotlights. Doctors never really had any good reasons not to engage with it, apart from a lack of understanding and awareness, but now… healthcare providers truly have no more excuses for their disregard of the available published literature on cannabinoids, terpenoids, and flavonoids, as well as the endocannabinoidome (say that 2 times fast! This is just the full playing field of stuff that is involved in the experience of cannabis, natural or from a plant), nor can doctors put aside open conversations about what patients are doing to care for themselves outside of the clinical office space, what they want to do better with their wellness, and how they’re achieving the results that they seek.
Softball Limitations and Oversights
Sampling Bias and Underreporting: The study comes up with a finding that lower socioeconomic status (SES) groups are reporting less cannabis use. This contradicts public health data see (here, here, and here) that suggests much higher usage in lower SES groups. To a Sherlock Holmes eye, this discrepancy might suggest either underreporting by those groups (as part of the LA health system in general or perhaps the groups of patients studied in this article, aka a sampling bias) as those surveyed might have better access to the healthcare system, or be more well-to-do than “typical” low SES groups.
Lack of Diagnostic Validation: One of the study's important limitations is the absence of diagnostic validation from primary care providers. This raises critical questions about the survey data's relevance and whether it accurately reflects clinically diagnosed conditions. It's puzzling that the researchers focused solely on self-reported data without corroborating it with information from patient visits. This oversight limits our understanding of the actual conditions being treated with cannabis. For instance, patients might report using cannabis for pain relief, but it could be part of a broader management plan for conditions like Crohn's Disease or arthritis. Similarly, reported sleep issues might be secondary to other underlying health problems. Without this diagnostic validation, the interpretation of cannabis use is restricted to symptom management rather than understanding its use in clinically diagnosed conditions, which could significantly alter the perceived value and risks of cannabis.
Legal and Cultural Context: The study's is set pulling data from California, with its unique legal and cultural environment. This limits the generalizability of the results. Also important to note, the data was collected during the COVID-19 pandemic, when the culture was largely encouraged (tacitly and overtly) to seek self-care, which may unnaturally boost the results, showing influenced cannabis use patterns, as people had less contact with the medical establishment and turned to self-care.
Data Gaps: The study misses 15% of the patient population who don't use the electronic health record system, representing a significant data gap (35k out of 235k). This is a big enough number that we have to fudge some of the other numbers to call them really distinct and meaningful from one another (we don’t have a full view).
Improving Patient-Doctor Communication
One key point bottom-line takeaway that the researchers seem to misunderstand, or don’t discuss, is the true goal of improving communication between patients and doctors regarding increased cannabis use. It's not just about preventing addiction, because we know that the rates of cannabis addiction are not different from baseline rates of human addiction to anything (exercise, binge-watching TV, caffeine, etc - see studies here, here, and here). Instead, the focus should be on helping patients achieve the symptom relief and clinical satisfaction they seek. These findings scream that the medical community in California isn't fully addressing the needs of their patients, who are turning to outside sources to get the relief they want.
This article was just featured in High Times by AJ Harrington. Check it out here:
https://hightimes.com/health/medical-marijuana/survey-finds-1-out-of-6-americans-use-weed-many-for-medical-reasons/